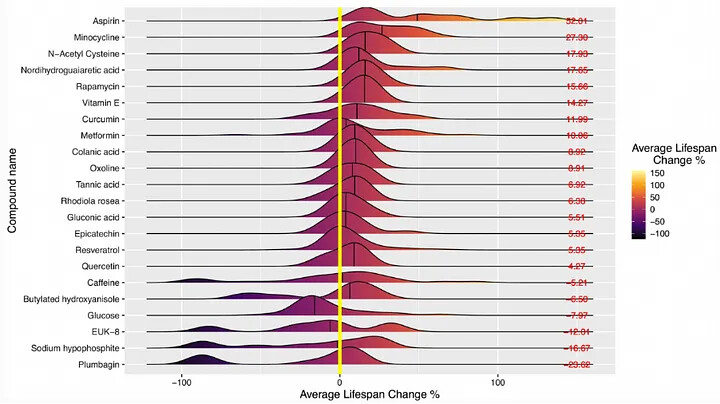
The current molecules most likely to work
Other Lists: ( ITP Test Results Thread | Diabetes and Glucose Control - Life Extension ). Note that mice die disproportionately of cancer, which biases ITP results (and may make some pro-survival/anti-dementia factors have weaker effects than they would in humans)
(the more supplements you take, the higher your chances of taking at least one that suppress your appetite by ~10-15% which alone induces metabolic benefits. Bryan Johnson has a good list). But increases risks of heavy metal contamination and bad synergies (semaglutide reduces need for half of them)
I want to be comprehensive in this post (cover as much as I can) so my post here is long, but the effect size of rapamycin+acarbose+canagliflozin is so so so SO much higher than any of the others listed here that a 90/10 would just involve those two and skipping the rest.
- retatrutide. Does not have induce nausea like semaglutide, so far more appropriate for intermittent dosing. Can halve dementia risk. Probably the most pro-longevity drug ever developed. Cremieux is a massive fan/
- GLP-1 agonists like Semaglutide. New Antiobesity Drugs Help People Shed Dozens of Pounds, but They Must Be Taken for a Lifetime | Scientific American Appetite suppressant. increases insulin (which you can reduce by rapamycin). Can induce fasting/calorie restriction/once-a-day feeding (tho hunger mediates SOME of the benefit of CR - https://www.cell.com/cell-reports/fulltext/S2211-1247(22)00608-8 ). Operates on ghrelin rather than leptin (safer this way b/c leptin induces ROS/tolerance). Stronger appetite suppression effects than anything else, may be good for losing visceral abdominal fat. You do not need to consistently be on it (people on trials regain much of their weight after stopping, but for those using it to reduce calories, the reduction in lifetime-integrated calorie consumption still holds). Intermittent (oral) Rybelsus / Semaglutide use in healthy individuals? - #26 by drsteve7777 - Rapamycin Longevity News . Decreases hemoglobin A1C more drastically than other drugs. Not ITP-tested b/c they need to figure out dosing. People often comment on how doing 2-4 day fasts (each month or several times a year) induces long-lasting metabolic shifts - this is the easiest way to do it even if you only do on occasion.Tirzepatide may be even better (though not on a mg-mg/price basis) and is a GIP agonist so it could strengthen osteoclasts. Then there is LY3437943. The doses needed for calorie reduction are smaller than those used in weight loss, so 0.5mg injections work. This is also the easiest way to decrease exposure to microplastics. Overall, I estimate the pro-longevity effect size of semaglutide to be higher than any other drug, including rapamycin. It also reduces the amount of other drugs you have to take due to overlapping mechanisms (I would still take taurine and plasmalogens)
https://www.nature.com/articles/d41586-024-00118-4 - may even act on inflammation independently of appetite reduction
Steve Austad bets on Ozempic + GH for the X-Prize…
(lift weights at least once a week to prevent reductions in muscle size, or take breaks in case body fat percentage goes too low)
-
rapamycin [10mg/week or 20mg/every 2 weeks - or https://twitter.com/Blagosklonny/status/1401976083038281734 ]. The gold standard with strongest pro-LS effects (outside of the other pan-MTOR inhibitors). IT IS POSSIBLE TO BUILD TOLERANCE TO RAPAMYCIN (you may want some breaks that are several weeks long). see a brian kennedy interview https://twitter.com/InquilineKea/status/1402449755234570244
take rapamycin with grapefruit to increase concentrations ESP if you’re male (males get lower increase in blood rapamycin with any given dosage). Patients who drank eight ounces a day of grapefruit juice increased their sirolimus levels by 350 percent
Daily dosing may be better than weekly dosing for preventing “rebound effects”. Higher doses may increase GlycanAge (small N)
CBD might also increase rapamycin levels.
Rapamycin may induce insulin resistance (https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC3384435/ ) and increase blood lipids (esp free fatty acids) and may work better if you transition to high-fat/low-carb or take metformin to reduce these increases. Rapamycin may increase LDL levels (you can suppress with NEXLIZET) and gluconeogenesis (you can suppress with metformin).
There are alternative mTOR inhibitors in research like pan-mTOR inhibitors (eg Dr. Joan Mannick — mTOR’s Role in Aging - Rapamycin Longevity News ) or the mTOR catalytic inhibitors that may be more effective than the rapalogs or allosteric inhibitors (they may also have no mTORC2 inhibition). Considering Pan-mTOR Inhibitors as Alternatives to Rapamycin – Fight Aging! . #118 - Lloyd Klickstein, M.D., Ph.D.: Rapamycin, mTOR inhibition, and the biology of aging - Peter Attia lists RTB101
-
alpha-glucosidase inhibitors like acarbose (eat when eating starch/sucrose heavy foods, esp beans/grains, to blunt the rise in glucose → postprandial glucotoxicity seems to cause harm way out of proportion to glucose AUC). Acarbose is more easily absorbed if you chew it into powder before eating (this is easy b/c it tastes okay).
Acarbose might work for fats, but does not work for low-sucrose fruits (https://www.quora.com/Does-acarbose-work-for-reducing-the-glycemic-index-of-fruit ). May mildly decrease metformin bioavailability. Works more quickly/instantly than SGLT2 inhibitors. (IMPORTANT) SGLT inhibitors are not a substitute for Acarbose - longevity - Rapamycin Longevity News. Synergizes with rapamycin. May possibly reduce calorie bioavailability.
Miglitol may be even better and is systematically absorbed. Miglitol activates UCP1 - HOWEVER - miglitol may inhibit GIP and weaken the bones. Voglibose is another one
- SGLT1/SGLT2 inhibitors like canagliflozin Canagliflozin for Anti-aging (part 2) - #2 by AlexKChen - sglt2 - Rapamycin Longevity News (see Attia’s interview of Austad) - https://www.youtube.com/watch?v=7eW1bQZ1TmA . (IMPORTANT) SGLT inhibitors are not a substitute for Acarbose - longevity - Rapamycin Longevity News notes that canagliflozin may inhibit intestinal absorption of glucose (thru SGLT1 inhibition) whereas empagliflozin may not do the same thing => reduces time needed between taking the drug and eating if you’re an impulsive eater like this duck) => the brain also has SGLT1 receptors and benefits more from canagliflozin. It’s possible that the selective SGLT2 inhibitors (aka non-canagliflozin ones) might not reduce the BG spike much in non-diabetic people (see more at https://www.nature.com/articles/s41598-023-33086-2, The promise of SGLT2 inhibitors - Works in Progress Magazine )
Canagliflozin also works as a senolytic (2024 paper even says its senolytic effects may be better than its anti-glycemic ones)
It may be a good idea to take breaks/take it “1/3” of the time b/c SGLT2 inhibitors can increase appetite/fatigue if taken for too long.
Sotagliflozin is the newest SGLT1+SGLT2 inhibitor and may be better than any of them (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8659196/ => also shows canagliflozin is preferred due to SGLT1 inhibition)
canagliflozin is much more effective at reducing postprandial glucose spikes in healthy volunteers than dapagliflozin - though dapafliglozin is still much cheaper and still makes one pee out enough glucose.
-
taurine. Anti-glycative agent. Even Martin Borsch Jensen called the June 2023 paper impressive. Pyridoxamine is also the most interesting understudied B6 vitamer and may reduce ghrelin increases from AGE consumption…
-
Nexlizet (bempedoic acid and ezetimibe) to reduce LDL (reduces alzheimer’s risk). Much safer than the statins (which interfere with geranylgeraniol pathway). The proteoglycans in the blood vessel walls of humans seem particularly prone to blood vessel damage, and taking out the primary causes of death in humans does a lot in practice even though LDL in theory doesn’t directly increase aging rate (as you can see in lucky people like Mahathir Mohamad) and there are SOME positive correlations between moderately high LDL and longevity at the population level (even though people with genetically low LDL seem to suffer from no issues, which is the strongest argument for Nexlizet and PCSK9i)
-
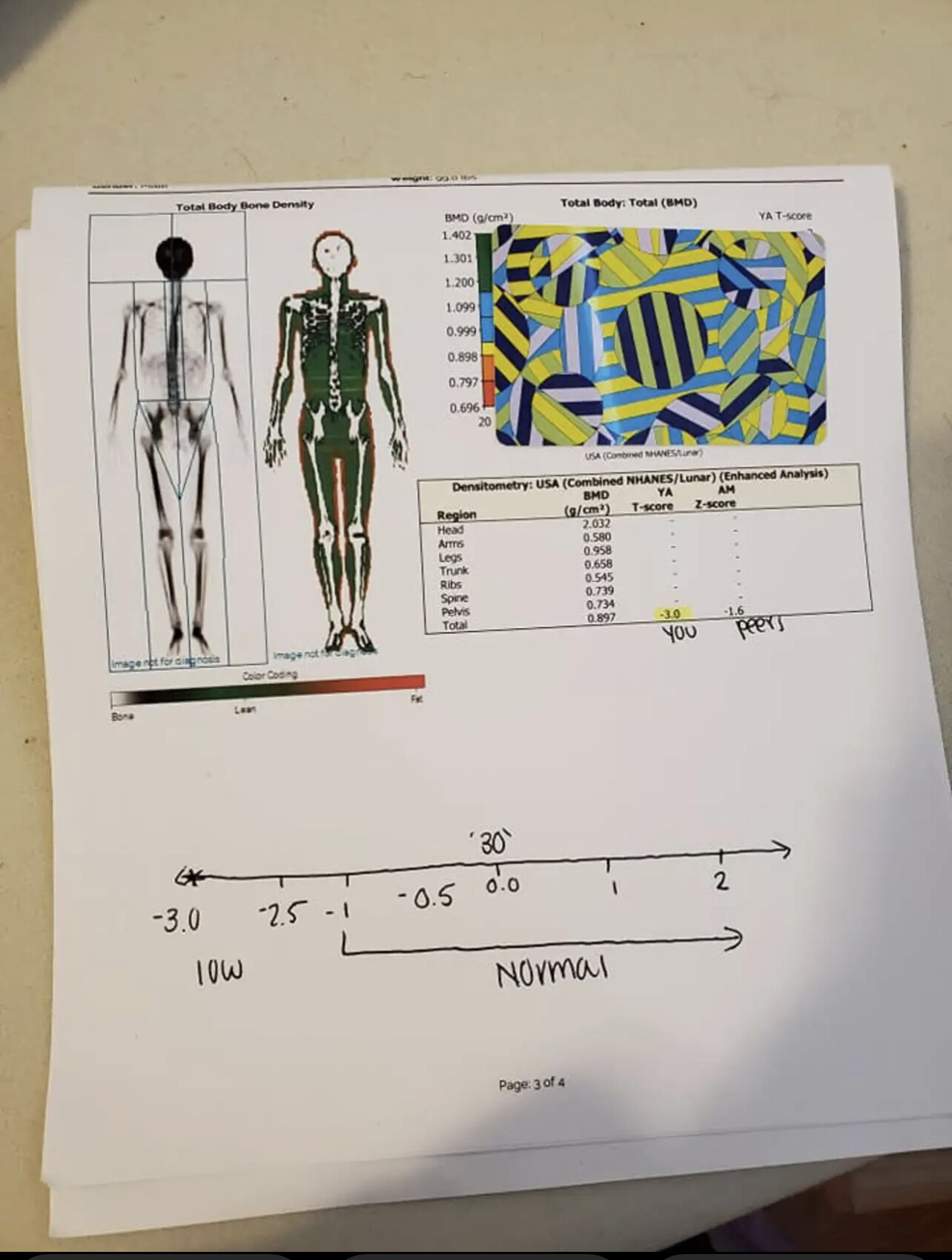
The bisphosphonate zoledronate, which has lots of strange other pro-longevity benefits. Many pro-longevity interventions, like veganism and calorie restriction - can lower bone density and zoledronate reduces much of that risk. Just take breaks after 2-3 years of use (that way reduces the temporarily increased risk of atypical femoral fractures) - but there are concerns with bisphosphonates making “rare bone microfractures” more common if used long term, especially if started earlier than most people start them. Zoledronate reduces cholesterol by acting 2-3 steps downstream of statins (also reduces protein prenylation). Since most non-human animals don’t die from arteriosclerosis or bone fractures, zoledronate increasing lifespan in non-human animals is EVEN MORE INTERESTING
-
Teriparatide Injection LATER IN LIFE - this is a bone-density increaser that ameliorates the primary downside of calorie restriction/frailty and has fewer risks than bisphosphonates). https://www.rapamycin.news/t/medications-for-low-bone-density-bisphosphonates-teriparatide-estrogens-potential-long-term-effects/4740 . It is a second-line treatment against osteoporosis, so insurance only covers it if you’ve failed BPs. The highest increases in bone density seem to come from combining different modalities (eg teriparatide + BPs or denosumab + BPs)
-
SARMs (eg S-40503 - Wikipedia) may be worth investigating
-
selegiline. Anti-Parkinson’s, may mildly help ADHD. Inhibits MAO-A (which produces H2O2 when breaking down catecholamines). Deprenyl - Anti-Aging Drug Proven Effective in Dogs - #10 by RapAdmin - longevity - Rapamycin Longevity News . 0.25 mg/kg works in older animals. https://archive.ph/deHMU . Kaeberlein said “evidence for selegiline stronger than for metformin”
-
C15:0 (look up fatty15.com). Odd-chained saturated fatty acids may help prevent lipid peroxidation.
-
gemfibrozil (PEPT1-blocker https://www.solvobiotech.com/transporters/pept1), see Brian kennedy ARDD2023. It might not have traditional fibrate activity
-
metformin. YES I know it has gotten a lot of “hate” for being “overrated” and for having slightly negative 90th percentile lifespan-effects - however - its haters have not considered synergies. https://www.youtube.com/watch?v=iByaqfmWfHQ . It synergizes well with rapamycin and counteracts “rapamycin-induced gluconeogenesis/insulin-resistance + increased blood lipids”. It ALSO synergizes well with empagliflozin. morten shows it decreases maximum lifespan (BY ITSELF). https://twitter.com/dweinkove/status/1564666004449419266 . Matt Kaeberlein later tweeted that it lifespan-synergizes well with a wide variety of compounds. ALSO, metformin at 1500mg/day CAN decrease appetite in some people, and that alone makes it longevity-relevant (the TAME study will use these doses). Take B12 to avoid homocysteine increases. It can reduce the hormetic/ROS-benefit from exercise, so don’t take it on days of heavy exercise. more here - Metformin and positive effects on epigenetic clocks - #64 by AlexKChen - Rapamycin Longevity News . Can reduce Horvath/Hannum epigenetic aging - though other studies may disagree. https://www.nature.com/articles/d41586-019-02638-w .
The “weak effects” may also be the result of “too low” dosing (though was the dosing used in ITP much higher than seen in humans?) “Significant dose‐dependent improvement in daily profiles of blood glucose was observed with metformin dosages up to 1,500 mg/day, with a trend towards further improvement observed at 2,250 mg/day” => there were very few humans on the highest dose, and (given the huge differences in relative blood concentrations of metformin seen between mice and humans) it’s likely that the ideal dose of metformin is higher than 2250 mg/day. Mice die disproportionately of cancer, and many cytoprotective mechanisms also protect cancer cells (ESPECIALLY if only started later in life). Pairing metformin with 14ppm rapamycin produced the highest longevity benefits of all interventions in ITP.
It can be a mild mitochondrial complex I inhibitor, which is my strongest concern (but does it do it at low doses, and does mild inhibition of complex I reduce mitochondrial ROS?) And - how does CR affect complex I? I will find out later.
metformin increases GDF15 which can reduce appetite AND associated with frailty (GDF15 is a weird hormone that seems to “stick out” in fraility assays).
Bryan Johnson of blueprint combines metformin with rapamycin with acarbose (he does not yet try the -flozins AFAIK)
A recent metformin study casts doubts on longevity indications => still on metformin monotherapy only (without concurrent rapamycin)
-
https://www.rapamycin.news/t/alpha-17-estradiol-another-top-anti-aging-drug/92 (MAY ELIMINATE THE GENDER DIFFERENCE IN LONGEVITY). ITP-approved. https://www.researchgate.net/publication/350211511_Cap-independent_translation_A_shared_mechanism_for_lifespan_extension_by_rapamycin_acarbose_and_17a-estradiol shows many similar pathways to CR even though this should act on more pathways than were studied in the ITP papers. Males have higher Glycanage (and OMICm age) than females - this could reduce the difference. Estriol (weak feminizing activity) and other estrogens (but avoid ethinylestradiol) can work too, esp in post-menopausal women. Also finasteride in men.
-
melatonin (decreases w/age and superpotent antioxidant that uniquely doesn’t even turn into a pro-oxidant after being oxidized). Amazon.com . This is the most potent antioxidant - if you can take it without it disrupting your sleep, you don’t really need others. See Doris Loh on everything about it. Doris Loh . Amazon.com . Melatonin megadoses? - #62 by desertshores - Rapamycin Longevity News and https://www.melatonin-research.net/index.php/MR/article/view/34 (see this for doses). Effects phase separation
Also, indole-based melatonin analogues
- rilmenidine - Rilmenidine Extends Lifespan and Healthspan by 20% - Rapamycin Longevity News. a blood pressure agent. Also sildenafil (idk about slowing aging rate, but it decreases the main causes of death)
- glycine. tastes slightly sweet/good - you can add the powder into your foods (WHICH MAKES IT IRRATIONAL NOT TO EAT IT). Can reduce appetite - Postprandial glycine as a biomarker of satiety: A dose-rising randomised control trial of whey protein in overweight women - PubMed . https://twitter.com/foundmyfitness/status/1376626837720162306 . maximize glycine to methionine ratio (ya this means collagen protein). ITP-passed (~8%). Can pair well with N-acetylcysteine. The most common building block of collagen. Might reduce homocysteine and methionine (https://onlinelibrary.wiley.com/doi/full/10.1111/acel.12953 )
Glycine is in fact an acceptor for methyl groups, and can in that way clear an excess of methionine. Too much methionine is not healthy: methionine is converted into homocysteine, a substance that has been associated with accelerated aging and aging-related disorders (R). Glycine can reduce methionine levels in the blood.
Astaxanthin has shown a variety of clinical benefits with good tolerability and safety. In double-blind, randomized controlled trials, it reduced oxidative stress by 5 mg or 20 mg/day in obese and overweight subjects and 5 mg, 20 mg or 40 mg/day in smokers [11, 12]. The results showed that oxidative DNA damage was inhibited, C-reactive protein and other inflammatory biomarkers were decreased, and tuberculin skin test immunity was enhanced [13, 14]. In another trial, daily astaxanthin doses of 6, 12, or 18 mg decreased triglycerides and increased HDL cholesterol and improved blood flow in microcirculation models
- glucosamine + chondroitin sulfate - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8441316/#acel13441-sup-0016, https://www.frontiersin.org/articles/10.3389/fragi.2021.741843/full (Amazon.com - which also has hyaluronic acid in it). glucosamine treatment increased collagen expression during aging (Figure S10, Table S6). Previous studies also implicated glucosamine supplementation in lifespan extension of C. elegans and mice (Weimer et al., 2014). Using our collagen reporter screening system, we determined that 20 μl/ml of hyaluronic acid and 400 μg/ml chondroitin sulfate prolonged collagen synthesis during aging and were sufficient to increase lifespan. Ewald also says it increases lost synthesis. If you want to look young for much longer, this is how to do it. Has a RR of 1.10 for cardiovascular disease in osteoarthritis patients…
- caffeine + modafinil or nicotine lozenges (for appetite suppression). Caffeine also boosts longevity in several model organisms, protects against dementia, extends telomeres in one study, and has weird pro-longevity effects across multiple pathways. https://www.frontiersin.org/articles/10.3389/fnins.2019.00263/full . Modafinil CAN increase mTOR in some people so take rap/met on top of it. Caffeine is also a phosphodiesterase inhibitor (+reduces inflammation) and increases lifespan in a surprisingly large number of studies.
- NAC (5g at a time, and now restricted). N-Acetylcysteine ethyl ester (NACET): a novel lipophilic cell-permeable cysteine derivative with an unusual pharmacokinetic feature and remarkable antioxidant potential - PubMed is at science.bio and more potent than NAC and more easily sucked up by cells b/c ethyl ester is more lipophilic than NAC with minimal amt of extra steric hindrance
- plasmalogens (see dayan goodenowe). Shark liver oil supplementation enriches endogenous plasmalogens and reduces markers of dyslipidaemia and inflammation — MED-LIFE DISCOVERIES. Get tested through opencures. https://www.eurekalert.org/news-releases/952176
- lutein/zeaxanthin/astaxanthin and other carotenoids. Decrease epigenetic age. Carotenoids Are Associated With A Younger Epigenetic Age And Reduced All-Cause Mortality Risk | Michael Lustgarten . Astaxanthin: A Potential Treatment in Disease and Aging, Lifespan Increase - #165 by RapAdmin - Rapamycin Longevity News . Doses used in supplements are very low compared to LS-extending doses
- green tea (in moderation, TOO MUCH can cause liver damage - Green Tea - LiverTox - NCBI Bookshelf ). epicatechin
- all the other molecules listed in ITP
- potassium. https://optimisingnutrition.com/nutrient-balance-ratios/#more-10808 . It helps satiate appetite, reduce blood pressure, and reduce calories consumed. It also neutralizes negative effects of excess sodium
- From Peter Attia: * “If we simply took this tool that exists, PCSK9 inhibitors, which have no side effects and obliterate apoB, and we started injecting them into people when they were 30 and taking everybody’s apoB when they were 30 down to 30 or 40 or 50 milligrams per deciliter, I would argue that ASCVD would be the 10th leading cause of death as opposed to the leading cause of death ”. Mice do not die of heart disease so this isn’t seen in ITP (In mice, more than 90% of the cholesterol in the blood is in HDL ). Unlikely to boost lifespan in the healthiest.
- SIRT6 activators (fucoidin). see Vera. Could decrease chromatin/epigenetic aging. https://www.youtube.com/watch?v=VGKaa7dh2vg
- FGF21 activators
- https://www.longecity.org/forum/stacks/stack/122-michaels-tiered-supplement/
- Vitamin K2 (most people are deficient). Natto is the best source (natto ALSO is rich in spermidine and genistein and one of the few individual foods individually associated with longevity)
MORE INTERESTING MAYBES
- Thioflavin T (anti-amyloidogenesis)
- https://www.brown.edu/news/2019-02-06/aging (particularly lamivudine for retrotransposons), esp b/c aging increases transposon/LINE1 activity => genomic instability. There’s a chance that this becomes almost as important as rapamycin/empagliflozin in older people b/c it acts on the most orthogonal pathway from them. Some antiretrovirals may interfere with telomerase (+there are uncertainties with mitochondria). https://en.wikipedia.org/wiki/Reverse-transcriptase_inhibitor . ORF2-degraders may be more effective (https://youtu.be/5eQi4NFH7mk?t=2772 ) b/c they inhibit both reverse transcriptase and endonuclease activities of LINE1. https://en.wikipedia.org/wiki/Zidovudine is an antiretroviral with suggestive evidence -
- deuterated water - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5108472/ (KIE - kinetic isotope effect). Even SMALL increases in D2O concentration can drastically reduce H2O2 levels. Deuterated amino acids also reduce carbonyl stress
- RT-001 (deuterated PUFAs at bis-allylic position [D’s at the middle C connected by TWO double bonds], see Retrotrope). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5108472/ . https://medium.com/@denis.odinokov/what-are-the-currently-available-methods-to-impede-the-accumulation-of-modified-long-lived-960aaa10bc2 . There was a medium post a few years ago I can no longer find… https://www.reddit.com/r/chemistry/comments/525wr1/deuterating_fatty_acids_to_treat_diseases/ . https://www.fightaging.org/archives/2015/10/a-brief-look-at-retrotope.php + https://www.reddit.com/r/longevity/comments/ck88do/mikhail_shchepinov_presenting_at_undoing_aging/
- SD-1077 (deuterated L-DOPA => deuterated dopamine).
- Deuterated Vitamin A (ALK-001)- https://iovs.arvojournals.org/article.aspx?articleid=2779035 (more for vision than longevity)
- https://www.authorea.com/users/478442/articles/566678-research-progress-and-synthesis-methods-of-deuterated-drugs
- exosomes [way more interesting than theothers, see kimera]. There are some skeptics - search rapamycin.news.
- BHB ketone esters (eg the one manufactured by Eric Verdin). Reduces glucose/triglycerides/free fatty acids (and appetite, and maybe sleep need too). More here https://www.rapamycin.news/t/your-experiences-using-supplemental-bhb-esters-to-reduce-blood-glucose-appetite-hdacs-slow-aging-etc/4973
- fullerenes like e,e,e-methanofullerene(60)-63-tris malonic acid (des-ignated C3), is a potent catalytic superoxide dismutase mimetic which has shown neuroprotective efficacy in a number of animal models of neurologic disease. See Laura Dugan. I’m still concerned about whether the C60 structure makes the molecule more likely to “get stuck” in the wrong places in the cell. See https://srconstantin.github.io/2018/05/04/fullerenes.html
- cannabinoids (can clear amyloid plaque). https://www.liebertpub.com/doi/10.1089/can.2020.0103 more useful in older people than in teens. https://www.longevity.technology/can-active-ingredient-in-cannabis-protect-against-brain-aging/?utm_source=ActiveCampaign&utm_medium=email&utm_content=Cometh+the+fasting+hour%2C+cometh+the+man&utm_campaign=Newsletter+-+Week04_2&vgo_ee=RPoQmCkvipD5QXRrFOmqPflMy%2BOWWuyaZunZiCXh6gI%3D . THROUGH autophagy - https://www.lifespan.io/news/cannabidiol-increases-lifespan-and-healthspan-in-worms/ . USE EDIBLES, do NOT smoke (excess smoking contaminates ALL the research in active cannabis users). ONE study shows they increase rapamycin levels (https://pubmed.ncbi.nlm.nih.gov/31924480/ ). Another study shows that they may reduce retinal nerve fiber thinning w/age. OF ALL THE MAYBES, I think these are the most important/easiest to access, but it will take years to obtain high-power studies on them in people who use them responsibly
- baking powder for inflammation and converting macrophages to less pro-inflammatory form (https://www.sciencedaily.com/releases/2018/04/180425093745.htm ). Also it seltzes which can suppress appetite a tiny bit.
- https://link.springer.com/article/10.1007/s13659-022-00339-y NEW 2022 LIST, like nitrones -https://pubmed.ncbi.nlm.nih.gov/11976206/ . N-tert-butyl-α-Phenylnitrone (PBN)
- https://en.wikipedia.org/wiki/Tafamidis (for TTX - see fightaging.org - it is often lifetime-limiting for centenarians). May be best in those who are not too old (similarly with the anti-amyloid antibodies). https://en.wikipedia.org/wiki/Wild-type_transthyretin_amyloid (25% of men over 80 may have it)
- cholinergics like donepezil can also suppress appetite and MAYBE preserve memory. They may also increase parasympathetic tone (maybe helping HRV)
- follistatin (esp good for reducing frailty in older people). Minicircle has experimental plasmid therapy (long-term risks are unknown). See fightaging for reference on one study showing its longevity effects. https://www.fightaging.org/archives/2021/07/telomerase-and-follistatin-gene-therapies-delivered-via-cytomegalovirus-extend-life-in-mice/ . HOWEVER, it inhibits GDF11 (see Steve’s YouTube on GDF11) and one nature paper ties it to increased insulin resistance. Reason @ FightAging has done the trial. They can increase appetite, however (whether this is downstream of increased muscle mass is unknown)
- bicalutamide to reduce testosterone (transgender people consider it superior to spiro - they have WAY more info on it). Testosterone accelerates epigenetic aging. Possibly unnecessary as 17-alpha-estradiol may be enough to eliminate sex differences in longevity.
- MEK inhibitor (trametinib) has not been tested in humans, but could synergize well with rapamycin+lithium (see A triple drug combination targeting components of the nutrient-sensing network maximizes longevity | PNAS ). MEK inhibitors inhibit a mTOR-independent downstream effect of BOTH thyroid hormone and growth hormone. HOWEVER, a friend of mine says “it has a lot of side effects in greater than 30% of patients including albumin imbalance, anemia, liver damage (ALT increase), and lymphedema”
LESS INTERESTING MAYBES
- atorvastatin [the only statin] - https://www.rapamycin.news/t/first-report-from-epiterna-on-the-search-for-drugs-that-can-extend-human-lifespan/12651
- estriol and estrone (among estrogens)
- omega-3’s like https://www.amazon.com/dp/B08F8K36RP?psc=1&smid=A3IQGL03Z0MNP5&ref_=chk_typ_imgToDp . Negative on ITP (but they probably improve healthspan and mindspan way more, and massively boost the average if not the maximum). Omega-3’s are also very easily oxidized, and animals with a higher % of omega-3-based lipids die younger (the relationship may not be everywhere monotonic)
- creatine (for vegans). May reduce homocysteine levels. Much of the body’s methylation enzymes are used to synthesize creatine, which prevents these methyl groups from reducing homocysteine + maintaining healthy DNA methylation (methyl donors help decrease DNAm age on sum)
- 4-phenylbutyrate
- quercetin + datasinib. Senolytics have larger effect sizes in the young (from what one person told me), and Morgan Levine is doing a trial to see their effect on epigenetic aging.
- ergothionine (in mushrooms). Mushrooms HELLA REDUCE the risk of cognitive decline. cell has a SPECIAL transporter for it, can be stored for ~1 month. https://archive.ph/oiwm2 . lustgarten says too high consumption can increase mortality (U shaped association). found most in oyster mushrooms
- GLYLO - https://www.biorxiv.org/content/10.1101/2022.08.10.503411v1 (even decreases appetite). The ingredients are so common and GLYLO is way more $$ than justified
- carvedilol (beta-blockers have risks, but are still net-positive sum and carvedilol has fewest metabolic effects - https://www.sciencedirect.com/science/article/pii/S0019483216000043 ). May be especially important if you take stimulants.
26The beneficial effects of carvedilol compared to metoprolol and atenolol on lipid parameters has been demonstrated in several small studies.13,25,27Carvedilol has selective α -1-adrenoreceptor blocking activity, causing vasodilation and a reduction in insulin resistance
- https://brain.forever-healthy.org/display/EN/Rejuvenation+Now (looks unlikely. See the database for the others)
- https://www.pnas.org/content/115/43/10836 . carnosine/(anti-glycation, helpful for vegans, unlikely to boost lifespan). https://www.biomolther.org/journal/view.html?uid=948&vmd=Full . In any case, metformin itself has potent anti-glycation effects. Taurine MIGHT enhance metformin’s effects on oxidative stress - https://supp.ai/i/metformin-taurine/C0025598-C0039350
- Vitamin C megadoses. Unlikely to boost lifespan in many people (and I know that Linus Pauling got a lot of hate after his death) but there are indications they can be useful in some populations, particularly older ones depleted in endogeneous antioxidant production (this is similar to Vitamin E - which can have negative effects on LS and yet JP Magalhaes produced a diagram showing otherwise). https://archive.ph/qKLqQ . Vitamin C can turn pro-oxidant in conditions of high Iron load. If you’re high-melatonin AND low iron, it can prevent Vitamin C from turning pro-oxidant.
- glutathione (MAY suppress endogenous production)
- psychedelics (esp shrooms/DOI/2CB) in SOME people (only b/c they seem to drastically improve emotional health in SOME people even after a few doses and emotional health helps w/lngevity). Shrooms may upregulate 5-HT2B which may increase risks of cardiac fibrosis. TAKE A 5-HT2B ANTAGONIST WITH THEM (qualiacomputing/andres gomez emilson knows more than I do on this)
- https://www.ergogenic.health/supplement-products/nacet-powder-supplement-n-acetyl-l-cysteine-ethyl-ester
- fisetin (in strawberries). see https://en.wikipedia.org/wiki/Glyoxalase_system
- methylene blue might be one. does not work in ITP
- https://en.wikipedia.org/wiki/N-Acetylmannosamine for reducing GlycanAge (increasing sialyation). Probably only useful in much older people
- lithium (Gsk-3 inhibitor, does not increase LS in mice [https://onlinelibrary.wiley.com/doi/full/10.1111/acel.13479 ], can synergize with MEK inhibitors in Drosophila). Reduces epigenetic aging rate in bipolar people [1] [2]
- tumeric/curcumin + piperine. turmeric also can possibly chelate iron. https://www.amazon.com/dp/B0001M10RE?ref=nb_sb_ss_w_as-ypp-ro-model_ypp_ro_model_k0_1_20&crid=1JG6XF57UJYTN&sprefix=indian+curry+seasoin has it all. https://www.youtube.com/watch?v=FtwDSU6caH8 . Unlikely to increase lifespan. Curcumin has HUGE polyphamarcology effects and may result in an unusually high level of false positives
- 3-hydroxyanthranilic acid - a new metabolite for healthy lifespan extension ((June 2021) https://doi.org/10.1101/2021.06.01.446651 )
- allicins (in onions)
- amino acid transport inhibitors
*sulforophane + myrosinase (see https://www.amazon.com/Jarrow-Formulas-BroccoMax-Supports-Delayed/dp/B0013OVTM0 ). Unlikely to be much of an effect - kaempferol > (myricetin, isorhamnetin) for dementia risk - https://www.medpagetoday.com/neurology/alzheimersdisease/84603
- apigenin (CD38 inhibitor) found in parsley
- sulforaphane (in broccoli sprouts) + activator
- high ORAC spices (eg cloves)
- alpha ketoglutarate [only in older people, I expect effect size to be small]. Brian Kennedy says very safe, people have taken up to 10mg/day (or 2% of their entire diet). No one knows why this is any more “special” than any krebs-cycle intermediate
- iron chelators (see Mindspan by Preston Estep)
- https://jarrow.com/products/boneup-240-capsules (many longevity interventions decrease bone density so you’ll need a backup plan). strontium also increases it but may have cardiac side effects. also see https://www.crsociety.org/topic/11344-benefits-vs-risks-of-strontium-supplements/
- NMN/NAD+ (unlikely to boost lifespan, but many people are deficient so test for deficiencies and if you are take it). https://www.youtube.com/watch?v=t3e24vYjiks says effects are weak at best, probably higher for healthspan. good source here - https://www.amazon.com/N-Stac-Nicotinamide-Mononucleotide-Bioavailable-Dual-Action-Support-Made/dp/B07YYP47TT/ref=sr_1_5?crid=2H6I2J83GBJG8&keywords=nmn+apigenin&qid=1649534638&sprefix=nmn+apigenin%2Caps%2C140&sr=8-5 . CD38 may have an important role despite reducing NAD+ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7422487/
- mulberry leaves/nettle leaves
- mixed tocopherols/tocophenols (NOT vitaminE)
- alpha lipoic acid and ALCAR
- spermidine (effect size very small, you can do rapamycin to way better increase autophagy)
- Hsf-1 and Hsp70 activators (Hsp70 activators may be net negative if your amyloid load is above a certain level in older ppl)
- https://www.rapamycin.news/t/anti-inflammatory-activity-of-tocotrienols-in-age-related-pathologies/1855/14
EARLY INTERVENTION MAY BE IMPORTANT THAN LATE INTERVENTION:
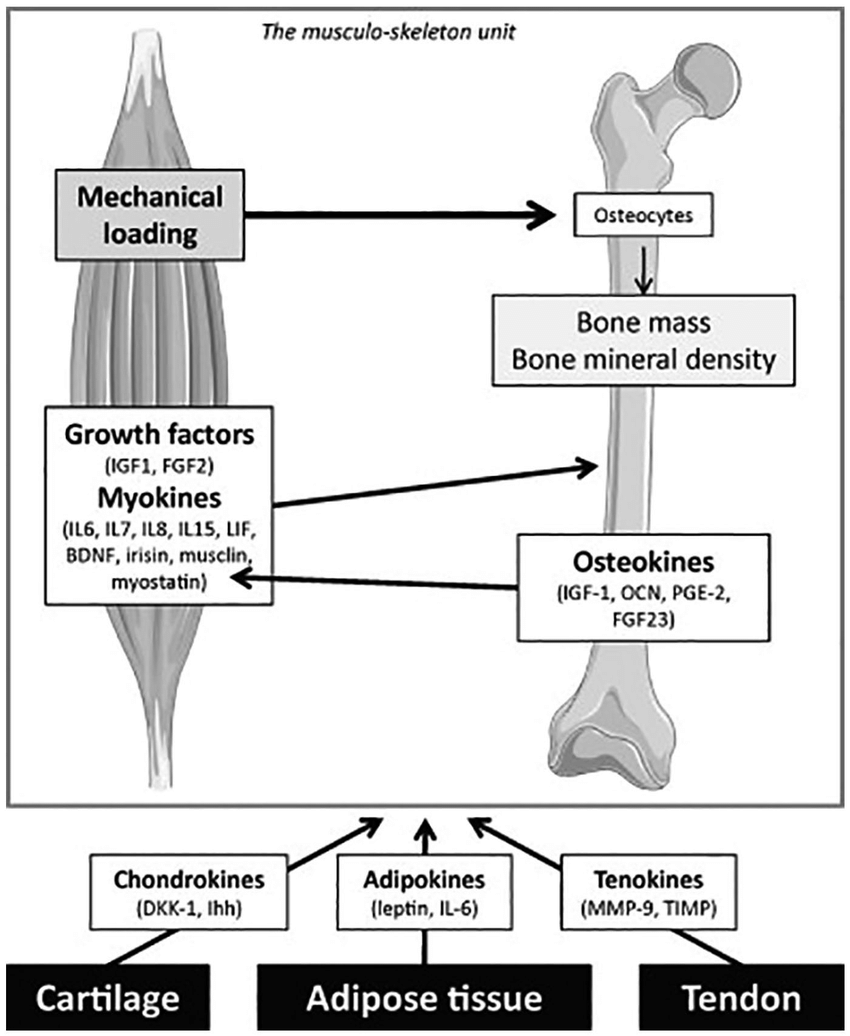
Taken together, the data presented here suggest that intervention with AAV-Kl may be more effective in slowing the progression of sarcopenia at an earlier timepoint, rather than rescuing advanced pathology, at which time the transcriptomic response to intervention appears to be more stochastic. An interesting area of future investigation includes the determination of whether network entropy and PPI network architecture may be predictive of the efficacy of therapies designed to counteract the effect of time on skeletal muscle health and function. As an extension of this work, it would also be interesting in future studies to determine whether upregulation of Klotho at a younger age could attenuate functional declines into old, and possibly even oldest-old, age
BE CAREFUL ABOUT HERBS/SPICES (EVEN GREEN TEA) - HERBS CAN CAUSE LIVER DAMAGE IF CONSUMED IN EXCESS (especially the ones that are very potent). If you use them, make sure to regularly measure liver enzymes and get heavy metal testing b/c herbs are often contaminated with lead/cadmium
Vitamins/minerals to supplement:
- Vitamin D (get levels at around 45-50 ng/dL)
- folate (methyl donor, decreases all cause mortality). https://www.crsociety.org/topic/17261-associations-between-146-nutrients-and-all-cause-mortality/?tab=comments#comment-39541
- betaine/trimethylglycine, also methyl donor, decreases homocysteine
- manganese (also decreases mortality, but I’d be careful about metals that aren’t zinc)
- magnesium (most people are deficient, it helps reduce calcium (neuro,mito)toxicity)
- zinc (see https://en.wikipedia.org/wiki/Metallothionein ). Zinc is one of the very few metals you want more rather than less of - it seems harder to change redox states than other metals
- creatine (esp if vegan) - can reduce homocysteine more robustly than betaine reduces it. https://www.foundmyfitness.com/topics/creatine#creatine-and-methyl-metabolism . read dayan goodenowe
NAD+ is worth looking into but doesn’t boost lifespan. See Brad Stanfield.
Experimental Small Molecules i’m most intrigued by XJB-5-131, deuterated PUFAs, and bendavia/SS-31 (SS-31 more for older than younger people - see Nathan Basisty presentation). There are so few lifespan studies on this (or even just epigenetic age studies on it). Go encourage VitaDAO people to stockpile these for studies!! YOU WANT TO PRESERVE CARDIOLIPIN STRUCTURE WITH AGE
DOI is a super-potent anti-inflammatory at low doses
Ones worth knowing about but which may not work:
cross-link breakers like ALT-711 and algebraiem. They may work better if administered earlier, just like the anti-beta-amyloid antibodies